How Human Biology Becomes Real-World Healthcare Practice in Medical Training
Medical school has a reputation for being relentless, but the volume of material is only part of the challenge. The deeper difficulty is learning to think with science, not just retain it. Medical education is built on the premise that foundational concepts in human biology do not exist as abstract theory but as the operational language of clinical work.
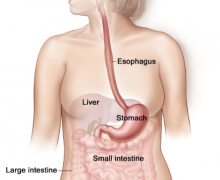
Human anatomy tells a clinician where to look. Physiology explains what should be happening and flags when it is not. Genetics shapes how a patient will respond to a diagnosis over time, and pharmacology determines which interventions are appropriate and at what dose. These disciplines are not studied in isolation; they are progressively layered throughout clinical training so that each new concept builds on the last.
What holds this structure together is clinical reasoning, the cognitive process by which scientific knowledge is translated into bedside decisions. A student who can recite a mechanism is not yet a clinician. One who can apply that mechanism to a patient’s presenting symptoms, history, and test results is beginning to practice medicine as it actually functions.
How Biology Is Applied in Medical Training
Medical education turns biology into practice through progressive application rather than isolated memorization. The foundational concepts in human biology, including human anatomy, physiology, genetics, and pharmacology, are each connected directly to diagnosis, treatment selection, and patient monitoring. Anatomy tells clinicians where to look; physiology tells them what to expect; genetics informs long-term risk; and pharmacology governs the choice and dosage of interventions.
Clinical reasoning is the mechanism that converts this scientific knowledge into bedside decisions. Rather than treating each discipline as a standalone subject, medical training weaves them together so that students learn to apply biological principles in the context of real patient presentations. The goal is not encyclopedic recall but functional, integrated thinking that holds up under the pressures of actual clinical work.
The Curriculum Builds from Systems to Patients
Why Basic Sciences Are Taught in Clinical Context
Medical education is not designed to teach biology first and medicine second. The curriculum is built to integrate them from the start, with learning objectives that anchor biological content to specific healthcare competencies rather than treating basic sciences as a preparatory phase to be completed before clinical work begins.
This design reflects decades of evidence that isolated memorization does not transfer well to patient care. When students learn renal physiology alongside fluid management decisions, or cell biology alongside diagnostic reasoning, the knowledge becomes functional rather than inert. The AAMC-HHMI report on scientific foundations for future physicians formalized this thinking by arguing that health sciences training should emphasize competency over content coverage, a shift that has since influenced how programs across premedical education and early medical school sequence their material.
Where Preclinical Learning Starts to Mirror Care
The transition from systems-level biology to patient-centered thinking rarely happens at a single point. Interdisciplinary curriculum design creates that shift gradually, with case-based learning, clinical vignettes, and structured problem-solving introduced well before students enter hospital settings.
Premedical education increasingly reflects this approach, with programs embedding clinical context into coursework so that students arrive at medical school with frameworks already oriented toward practice. Competency-based curricula often extend beyond conceptual mastery into assessment readiness for patient-care roles; effective CCMA exam prep, for instance, reflects this same philosophy at the allied health level, where applied competency is assessed alongside foundational knowledge. The continuum matters because clinical readiness is built incrementally, not delivered at graduation.
Clinical Reasoning Turns Science into Decisions
Physiology and pathology do not become useful at the moment a student memorizes them. They become useful when a student can apply them to a patient who presents with overlapping, sometimes contradictory symptoms, and use that knowledge to build a working differential.
Clinical reasoning is the process that makes this possible. When a patient reports chest pain and shortness of breath, it is physiological knowledge that helps a trainee distinguish between cardiac, pulmonary, and musculoskeletal causes. Each possibility carries a different biological mechanism, and ruling one out requires knowing what that mechanism would and would not produce.
Pharmacology and genetics add further dimensions to this reasoning. A treatment that is appropriate for one patient may carry elevated risk for another based on genetic variants that affect drug metabolism, meaning the clinical decision is never purely symptom-driven. This is why clinical training consistently returns to applied scenarios rather than isolated theory. A student who can explain a receptor pathway in the abstract has not yet developed clinical competency; that competency emerges when the same student can connect that pathway to a prescribing decision, a contraindication, or a change in a patient’s observed response.
Simulation Is Where Concepts Become Skills
As the curriculum moves students closer to patient contact, simulation provides the critical bridge between knowing and doing.
What Students Practice Before Patient Contact
Simulation-based medical education creates a controlled environment where biological knowledge is rehearsed repeatedly before any contact with live patients. Anatomy, physiology, and infectious diseases all feature in structured scenarios that require trainees to act on what they know, not simply recall it.
A student working through a simulated emergency response must integrate cardiovascular physiology, pharmacology, and clinical reasoning simultaneously. The scenario does not advance because a trainee can define a concept; it advances because they can apply it under pressure. Clinical training that relies solely on lectures and textbooks leaves a gap between knowing and doing, and simulation is specifically designed to close that gap by forcing active application within a setting where errors carry no patient risk.
Why Simulation Improves Transfer to Practice
Repetition, structured feedback, and controlled conditions are what make simulation effective as a transfer mechanism. When a trainee works through the same scenario multiple times with corrective feedback at each stage, the biological concepts embedded in that scenario become procedural rather than declarative.
Research findings link simulation-based medical education to measurable gains in clinical skill performance and improvements in patient safety outcomes, consistent across specialties and skill levels. What simulation ultimately does is convert abstract biological knowledge into repeatable, observable clinical behavior, which is precisely what medical education must produce before a trainee enters supervised patient care.
Genetics Now Shapes More Personalized Care
Genetics has moved from a foundational science into an active instrument of clinical decision-making. Where it once primarily explained disease inheritance, it now informs risk stratification, diagnostic precision, and therapy selection in ways that vary meaningfully from one patient to the next.
This shift has reshaped how medical curricula treat the subject. Programs affiliated with institutions like Harvard Medical School have expanded genomics content beyond classical heredity to include pharmacogenomics, gene expression, and population-level variation, equipping trainees to interpret genetic data as part of routine clinical reasoning. The connection to personalized medicine is direct: when two patients present with the same diagnosis but respond differently to the same treatment, genetic factors frequently explain the divergence.
Trainees who have engaged with genomics through the lens of scientific advancements reshaping modern medicine are better positioned to apply this reasoning at the individual level. Public health benefits from this as well, since identifying genetic risk patterns within populations allows for earlier intervention and more targeted prevention strategies.
Why This Matters for Modern Healthcare
Medical education exists to close the distance between biological science and patient outcomes. When curriculum is designed around that goal, foundational content in anatomy, physiology, and genetics does not remain academic; it becomes the basis for clinical decisions that directly affect how patients are diagnosed, treated, and protected from harm.
The link between disease prevention and applied biology runs through every stage of training. Public health strategies depend on the same scientific literacy that guides individual patient care, which is why curriculum design choices at the medical school level carry consequences well beyond the classroom.